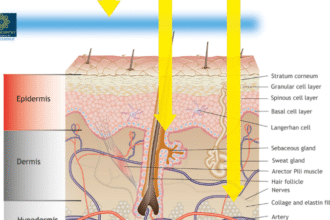
Long before European medical schools taught obstetrics as a specialty, Muslim physicians in the Islamic Golden Age were performing cesarean sections, describing uterine contractions, inventing surgical instruments, and establishing the world’s first comprehensive approach to childbirth. Their knowledge, shockingly, remained the standard of care for over 800 years.
Introduction: The “Dark Ages” That Weren’t Dark
When most people think of medicine before the Renaissance, they imagine bloodletting, superstition, and ignorance. European historians have long called the period between the fall of ancient Greece and the Italian Renaissance “The Dark Ages”—as if civilization itself had paused.
But while Europe slumbered, a brilliant flame burned elsewhere. From the 7th to the 13th centuries, the Islamic world experienced a Golden Age of science and medicine. Scholars in Baghdad, Cordoba, Cairo, and Bukhara translated Greek, Persian, and Indian manuscripts—then went far beyond them, adding original observations, correcting ancient errors, and inventing entirely new approaches to healing.
Nowhere is this forgotten legacy more striking than in the field of obstetrics—the care of pregnant women and childbirth.
A 2022 review published in Reproductive Sciences by Drs. Hossam and Eman Fadel documents, with remarkable detail, how early Islamic physicians fundamentally understood the birthing process in ways that would not be rediscovered in the West for centuries.
This article brings their story to a general audience.
Part 1: A Revolution Before the Renaissance
The Islamic Golden Age (approximately 700–1300 CE) was driven by a simple but powerful idea rooted in Islamic teachings. The Prophet Muhammad (peace be upon him) said:
“Allah has sent down both the disease and the cure, and He has appointed a cure for every disease, so treat yourselves.” (Hadith, Sunan Abi Dawud)
This commandment to seek healing—rather than to passively accept illness as fate—spurred generations of Muslim scholars to pursue medical knowledge with extraordinary dedication.
Within two centuries, they had:
- Translated Hippocrates, Galen, and Aristotle into Arabic.
- Corrected many of Galen’s errors (based on actual clinical observation).
- Written original encyclopedias that would be used in European universities until the 18th century.
Among the giants featured in the review: al-Razi (Rhazes), al-Zahrawi (Albucasis), al-Majusi (Haly Abbas), ibn Sina (Avicenna), al-Baladi, and ibn Maimon (Maimonides).
And here is a fact that may surprise you: Obstetrics and gynecology became a separate medical specialty under Islamic physicians—nearly 1,000 years before European medicine formally separated gynecology from general surgery in the early 19th century.
Table 1: Key Early Islamic Obstetricians and Their Major Contributions
| Physician | Lived (CE) | Major Work | Contribution to Obstetrics |
|---|---|---|---|
| al-Majusi (Haly Abbas) | d. 994 | Kamil al-Sina’ah (The Complete Medical Profession) | First to describe uterine contractions as the cause of delivery (not the fetus “swimming out”) |
| al-Razi (Rhazes) | 841–926 | al-Hawi (The Comprehensive Book) | Described malpresentations, cord around neck, internal podalic version; noted fever causes fetal death |
| al-Zahrawi (Albucasis) | 936–1013 | al-Tasrif (30 volumes) | Over 200 surgical instruments designed; detailed every malpresentation; described craniotomy, shoulder dystocia, placenta accreta |
| ibn Sina (Avicenna) | 980–1037 | al-Qanun (The Canon) | Complete classification of dystocia (maternal, fetal, uterine, placental causes) that mirrors modern classification |
| al-Baladi | early 11th C | Tadbir al-hawamil (Management of Pregnant Women) | First separate book on prenatal care; diet, exercise, sexual activity advice during pregnancy |
| ibn Maimon (Maimonides) | 1135–1204 | Medical Aphorisms | Described pica (food cravings), breast changes as abortion sign, milk as best newborn nutrition |
Part 2: Before They Knew—A Fundamental Discovery About Labor
Imagine practicing medicine without knowing what actually causes a baby to be born.
Before the Islamic physicians, that was exactly the situation. Hippocrates (the “Father of Medicine”) believed that the fetus simply swam or hatched its way out of the womb, like a chick breaking out of an egg. Even Galen, the most influential physician of the ancient world, had no real understanding of the mechanics of labor.
Then came al-Majusi (died 994 CE). In his book Kamil al-Sina’ah al-Tibbiyyah (The Complete Medical Profession), he made an observation so obvious in retrospect—but so revolutionary at the time: Uterine contractions push the baby out.
That single insight transformed obstetrics from guesswork into a physical, mechanical science. Now, physicians could understand why labor progressed or stalled. They could identify weak contractions, recognize obstructed labor, and intervene rationally.
Part 3: Al-Razi—The Clinician Who Wrote the Book on Pregnancy
Abu Bakr al-Razi (841–926 CE) was one of the greatest clinicians of any era. His massive encyclopedia al-Hawi fil-Tibb (The Comprehensive Book) was translated into Latin as Liber Continens and remained a standard text in Europe for 400 years.
In the third volume, he devoted an entire section to diseases of pregnancy, labor, and delivery. Here are some of his findings—every one of them as true today as 1,100 years ago:
On fetal position and timing
- “Fetuses born before the eighth month commonly present with the breech and usually die.” (We now know that prematurity and malpresentation are linked.)
- “The fetus changes its position from breech to vertex in the eighth month because the head is the heaviest part.” (A correct description of natural version.)
- “If the foot or the hand presents, it can cause death of the fetus and mother.” (This describes transverse lie and obstructed labor—a medical emergency even today.)
On twins
- “Twins are delivered within a few days of each other at the most.” (This corrects the ancient myth that twins could be born weeks apart.)
On initiating labor
- “Sexual intercourse brings on labor and facilitates delivery.” (Modern science explains this: seminal fluid contains prostaglandins, which ripen the cervix and trigger contractions.)
On fetal distress
- “Acute fever of the mother can cause fetal death.” (We now know that maternal hyperthermia and severe infections can indeed be fatal to the fetus.)
- “If the breast undergoes regressive changes, the fetus will die.” (Breast regression during pregnancy suggests severe placental insufficiency and low prolactin—a bad sign.)
On examining the laboring woman
Al-Razi instructed midwives to check the cervix—how dilated it was, what part was presenting, and to follow progress until full dilation. Only then should the woman be asked to push. This is exactly what modern obstetrics teaches.
On complications
He described umbilical cord around the neck as a cause of difficult labor and fetal death. He gave prescriptions of medicinal herbs to “facilitate” labor. And he described internal podalic version (turning the baby by reaching inside the uterus) and destructive operations to deliver a dead fetus when necessary.
Part 4: Al-Zahrawi—The Surgeon Who Invented Obstetric Instruments
Abu al-Qasim al-Zahrawi (936–1013 CE), known in the West as Albucasis, was born near Cordoba, Spain—then the glittering capital of Islamic Andalusia. His great work al-Tasrif (often translated as The Method of Medicine) consists of 30 volumes. Chapters 74 through 78 are devoted entirely to obstetrics and gynecology.
Al-Zahrawi did something no one before him had done systematically: he illustrated his surgical instruments. Over 200 of them are drawn in al-Tasrif, many of his own design. These images, when translated into Latin, would form the basis of obstetric instrument design in Europe for centuries.
What did he describe in labor management?
All possible malpresentations. He listed:
- Prolapsed hand or arm
- Incomplete breech (feet only)
- Complete breech (feet and buttocks)
- Transverse presentation (baby lying sideways)
- Cord around the neck
For each, he gave detailed maneuvers to correct the problem: replacing the hand, internal podalic version, changing the mother’s position, shaking her, placing her in a special delivery seat.
Non-surgical methods first
Al-Zahrawi was not reckless. He tried simpler measures first:
- A warm bath with mucilage of fenugreek and oil
- Valsalva maneuver (bearing down)
- Changing positions repeatedly
Only if these failed would he proceed to instruments.
Multifetal pregnancy
He correctly noted that twins are commonly born alive; triplets or quadruplets sometimes survive; but higher-order multiples are usually miscarried early. He also distinguished between twins sharing one sac (monochorionic) and twins in separate sacs (dichorionic)—a distinction modern ultrasound still makes.
Destructive operations for a dead fetus
Al-Zahrawi described these procedures with extraordinary clarity. Here is a condensed version of his instructions (translated by Spink & Lewis, 1973):
“If the fetal head is large and tightly squeezed, or if there is fluid in the head (hydrocephalus), introduce a spike-shaped scalpel (perforator) and split the head to let the water out, or smash it with the instrument called mishdakh (crusher, modern cranioclast). Then draw out the bones with forceps.
If the head comes out but the shoulders are stuck (shoulder dystocia), make an incision (cleidotomy). If the thorax is impacted, perforate to let out fluid (hydrothorax). If the belly is swollen with fluid (ascites), open it and drain.
If the fetus presents sideways (transverse) and you cannot turn it, cut it away piecemeal (evisceration) and extract it.”
These descriptions are graphic but also accurate. Before modern cesarean sections and anesthesia, such procedures were the only way to save a mother’s life when the fetus was already dead and obstructed.
On the placenta
Al-Zahrawi stressed: “It is necessary that not a scrap of the afterbirth be left behind in the womb.” He described methods to deliver the placenta: first, make the woman sneeze with her mouth and nose closed. If that fails, use vapors introduced into the uterus. If that fails, perform manual removal—gently separating the placenta from the uterine wall and pulling side to side, avoiding violent pulling that could cause uterine rupture or inversion.
He recognized that sometimes the placenta will not separate at all (today we call this placenta accreta). In that case, he advised stopping the maneuver and injecting an ointment to cause the placenta to putrefy over several days, after which it would loosen and come out. This is a primitive but logical approach before the era of blood transfusion and hysterectomy.
Abdominal pregnancy
Al-Zahrawi described a case of a pregnancy that was not in the uterus at all (ectopic abdominal pregnancy). It was mistaken for a dead intrauterine fetus. The extrauterine sac turned into an abscess, drained spontaneously, and eventually the bones of the dead fetus extruded. With proper wound care, the woman survived for a long time. This is a remarkable case report for the 10th century.
Al-Zahrawi’s Obstetric Instruments (Then and Now)
| Arabic Name | Translation | Modern Equivalent |
|---|---|---|
| Midfaa | Thruster | Obstetrical forceps (conceptually) |
| Mibdaa’ | Scalpel | Surgical scalpel |
| Mishdakh | Crusher | Cranioclast / cephalotribe |
| Sinnarah | Hook | Crotchet (obstetric hook) |
| Miqass | Scissors | Scissors (for episiotomy or cleidotomy) |
| Kalalib | Claws | Obstetrical forceps / grasping instrument |
*Source: Al-Zahrawi’s al-Tasrif, via Spink & Lewis translation, 1973*
Part 5: Ibn Sina (Avicenna)—The Genius Who Classified Everything Wrong With Labor
Ibn Sina (980–1037 CE) is perhaps the most famous physician of the Islamic Golden Age. His al-Qanun fil-tibb (The Canon of Medicine) was the standard medical textbook in European universities until the 17th century—500 years after his death.
His contribution to obstetrics was not a single discovery but an entire framework. He correctly noted that labor begins when the fetus can no longer get enough blood from the placenta—a theory modern research supports (placental function declines near term, triggering labor).
But his greatest achievement was his classification of dystocia (difficult labor). He broke it down into causes that are maternal, fetal, uterine, placental, timing-related, or due to midwife error.
Maternal causes
The mother may be weak, sick, undernourished, a first-time mother, too scared, elderly, obese, unable to push effectively, restless, or impatient with pain. Also: bladder tumors, urinary retention, rectal tumors, impacted hard stool.
Fetal causes
Female gender (he believed female fetuses were larger? This is not correct), big size, large head, too small (light) to descend properly, anomalies (double head), death (cannot help delivery), malpresentation (breech, transverse, prolapsed arm), and multifetal pregnancy.
Uterine causes
Small size (he is probably referring to a contracted pelvis—a key cause of obstructed labor), improperly healed cervical tear, or “hemorrhoids” of the uterus.
Placental causes
Thick placenta (accreta or previa?), premature rupture of membranes, “dry” uterus (oligohydramnios) making the birth canal less slippery.
Remarkably, this classification nearly mirrors our current understanding of the causes of difficult labor.
Ibn Sina also described management: for transverse lie, try manipulation first; if that fails, use hooks (kalalib); if that fails, eviscerate the dead fetus. He warned that if labor lasts more than four days, the fetus must be dead—and immediate extraction is needed before the dead fetus swells and rots, making delivery even harder.
He is also credited with being the first to associate prolonged obstructed labor with persistent urinary incontinence (vesico-vaginal fistula)—a devastating complication that still occurs in parts of the world today where emergency cesarean section is unavailable.
And here is a stunning fact: Avicenna recommended the use of both the fillet and forceps—centuries before their “invention” in Europe.
Part 6: Al-Baladi—The Father of Prenatal Care
While other physicians focused on labor and delivery, al-Baladi (early 11th century CE) wrote an entire book titled Tadbir al-hawamil—The Management of Pregnant Women, Children, Boys, and the Management of Their Diseases. This is arguably the first separate text on prenatal care in history.
His observations are wise and compassionate:
- Fetal health depends on the mother’s health. Active, healthy women with good digestion and mood tend to have strong, healthy fetuses.
- Milk secretion before delivery indicates fetal weakness.
- Pregnant women need more nutrition—but not too much, and the increase should be gradual with easily digested foods.
- More nutrition means more exercise (to balance the caloric intake and maintain fitness).
- Avoid jumping, carrying heavy loads, stooping, loud noises (like thunder), and traumatic events—all of which can cause miscarriage.
On sexual activity during pregnancy
Al-Baladi advised against complete abstinence, which he thought would cause difficult labor and stronger pains. But he also cautioned against too-frequent sex. He suggested avoiding intercourse in the first two months and after the sixth month—because in the last trimester the fetus is heavy and “cannot be trusted to fall during intercourse.” This advice is strikingly similar to what modern obstetricians tell women with a history of miscarriage (avoid sex in first trimester) or preterm labor (avoid sex in last trimester).
On common pregnancy complaints
He recognized morning sickness (nausea, vomiting, stomach upsets) and recommended dietary management. He discussed waham (cravings) and increased salivation (sialorrhea)—both very real symptoms of pregnancy.
Part 7: Ibn Maimon (Maimonides)—The Jewish Physician in the Sultan’s Court
Musa ibn Maimon (1135–1204 CE), known as Maimonides, was a Jewish theologian, philosopher, and physician born in Cordoba. He eventually became the chief physician to Sultan Saladin in Cairo.
His Medical Aphorisms includes a chapter “Doctrines Pertaining to Female Disorders.” He:
- Described pica (craving for non-food items) as due to “bad juices in the folds of the stomach,” which subside by the fourth month as vomiting clears them.
- Noted that shriveled breasts forebode abortion. “If pregnant with twins and one breast shrivels, she will abort one of the fetuses.”
- Observed that the pulse becomes stronger, more rapid, and fuller during pregnancy—all correct.
- Stated that breast milk is the most suitable nutrition for the newborn—a truth that modern pediatrics has only recently fully re-embraced after centuries of formula feeding.
Part 8: Women in Medicine—The Forgotten Midwives and Healers
The Islamic Golden Age was not exclusively male. Women were actively involved in the practice of medicine, especially in labor and delivery. They were called dayas (midwives). Most worked under the supervision of male physicians, but many were independent.
Ibn Zuhr (Avenzoar) , a renowned physician of Seville, had a daughter and granddaughter who became the first known female obstetricians in history.
In the 13th century, illustrations exist of a woman performing gynecologic surgery and another extracting a hydrocephalic dead fetus. Women healers in Egypt and the Ottoman Empire held salaried positions in medical institutions—a level of professional recognition that would not be matched in Europe for many centuries.
Conclusion: Why This Story Matters
European historians long labeled the medieval period “The Dark Ages,” effectively erasing the magnificent scientific civilization that flourished in the Islamic world. Only recently have scholars begun to uncover and report the truth.
As the historian M.S. Spink wrote in 1937—and as this 2022 review reaffirms:
“Attention is specially drawn to the gynecological and obstetrical instruments used by the Arabian doctors. It is shown that, in this branch at least, the Arabians were by no means wholly dependent upon the Classical writers … They altered and improved, out of recognition, the ideas they received from classical sources.
The speculum, the forceps, the lever and the crotchet mark in a special way the original Arab genius. It is also shown that the Arabs had developed a clear practical idea of what is normal, of what varieties of abnormality were to be met with, and by no means least, of prognosis, in obstetrical practice.”
The next time you hear about a woman receiving modern obstetric care—with forceps, cesarean section, or manual placental removal—remember: the knowledge that saved her life was, in many cases, first discovered, described, and taught in the Islamic Golden Age, more than a thousand years ago.
Reference: here
Other Articles: